
What is Crohn’s disease?
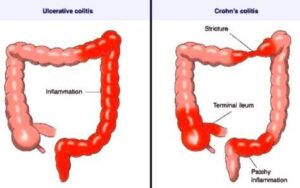
Crohn’s disease is a form of chronic inflammatory bowel disease (IBD) in which there are patches or segments of inflammation in any portion of the digestive tract from the mouth to the anus. The inflammation in Crohn’s disease is most often located in the lower part of the small intestine (the terminal ileum) and the upper portion of the large intestine. The inflammation of Crohn’s disease can involve all of the layers of the intestine. This inflammation can cause either narrow areas in the intestine called strictures, or tunnels through the intestine wall called fistulas, which may connect with other parts of the intestine or with the skin.
Who gets Crohn’s disease?
Doctors see only a small number of new cases each year, but because there is no cure, about three-quarters of a million Americans have the condition. It most commonly shows up between the ages of 10 and 40, with a second peak in people in their 60s. Crohn’s disease is more common in developed countries than developing countries. The incidence (rate of occurrence) has been increasing for several decades. There is some tendency for Crohn’s disease to run in families, but many patients have no relatives with the same condition. Men and women are equally affected.
What causes Crohn’s disease?
The exact cause is not yet known. It seems to be a combination of genetic and environmental factors that make a person’s immune system response become overactive. (The immune system response is the body’s defense against bacteria, viruses and other harmful substances.) This overactive response causes inflammation of the gut. There is no clear evidence that a specific diet or life stressor causes Crohn’s disease.
What are the symptoms of Crohn’s disease?
Most people who have Crohn’s disease have unpredictable flares of symptoms, often related to active disease or inflammation, separated by periods of no symptoms. During flares, patients can suffer diarrhea, weight loss and abdominal cramps or pain. Blood in the stool is less common in this form of IBD than it is with another form of IBD called ulcerative colitis, but it can happen.
How is the diagnosis of Crohn’s disease made?
Blood and stool tests are a common part of the evaluation, but there is no single blood or stool test that can enable a definite diagnosis. Crohn’s disease generally is diagnosed through a combination of colonoscopy and imaging tests.
Colonoscopy is a procedure that uses a small camera attached to a lighted, flexible tube inserted into the rectum to examine the entire colon and often the terminal ileum. Medicines are given to keep the patient comfortable. Tiny pieces of colon tissue are removed to examine under a microscope. This is called “biopsy” and is not painful.
Crohn’s disease also can be seen by other imaging tests; for example, computed tomography (CT) scan, magnetic resonance imaging (MRI) or barium x-rays. In general, the imaging tests are done without a hospital stay or any sedative medicines.
What is the treatment for Crohn’s disease?
Crohn’s disease is treated with a variety of medicines and often with surgery. Unfortunately, medical science does not have a cure. The goals of treatment are to decrease the inflammation in the intestines and to prevent flare-ups of symptoms, as well as to prevent complications from this condition. Steroid medicines such as prednisone may be used for short-term treatment, but because of side effects, avoiding long-term use of steroids (and narcotic pain medicines) is among the goals of treatment.
Some patients benefit from medications called immunomodulators, which act to “turn down” the immune system response. These are similar to medicines used to prevent a person’s immune system from rejecting an organ transplant. Azathioprine, 6-mercaptopurine and methotrexate are the most commonly used drugs in this group.
Many patients are treated with specially developed medicines called biologic therapies that may be given as shots or as infusions through an intravenous (IV) line. Many IBD specialists have a treatment center where patients can go to have medicines infused for a few hours and then return home. It is common to use an immunomodulator along with a biologic therapy.
Many people with Crohn’s disease will need surgery of some kind over their lifetime. Strictures may need to be treated by stretching the opening during endoscopy or colonoscopy, or by surgery to remove the narrow segment of intestine. Similarly, fistulas (tunnels from the intestine to other areas) that do not close in response to medication can sometimes be treated with endoscopy, but more often require surgery. This can range from placement of elastic tubing or stitches designed to help a fistula heal to removal of affected sections of the intestine. There are currently no routine endoscopic treatments for severely inflamed segments of intestine that fail to heal with medication, and surgical removal of these segments may be necessary.
While no particular diet has been shown to work for reducing symptoms of Crohn’s disease, some patients can develop low levels of iron, vitamin B12, or vitamin D and may need to take supplements of these or other vitamins and minerals to return levels to normal. Patients are encouraged to have a healthy, balanced diet and to keep up with vaccinations for conditions like the flu and pneumonia. Smoking is especially bad for patients with Crohn’s disease and can lead to an increased risk of needing surgery for their condition. Patients who smoke should quit.
Are there complications from Crohn’s disease?
Most people with Crohn’s disease do not have any complications, but for some it may lead to bleeding, intestinal blockage, or pockets of infection called abscesses. Minor cases of infection are usually treated with oral antibiotics and do not require admission to the hospital. Abscesses may need to be drained. Crohn’s disease can also lead to abnormal conditions elsewhere in the body. These may include certain skin conditions, particular kinds of arthritis and some eye problems. Longstanding Crohn’s disease can increase the risk of certain tumors, including skin and colon cancer. Patients should keep up to date on skin exams, pap smears, colonoscopies and other checkups.
General reminders:
Most patients with Crohn’s disease live full, productive lives and have healthy children. Since we do not yet have a cure for the condition, it is very worthwhile for people with Crohn’s disease to take an active part in their care, to follow medical advice and to keep personal copies of their medical information and test results. This can be done electronically, but paper records are also helpful.